Scientists have compiled the largest database of ancient DNA based on the bones and teeth of almost 5,000 humans who lived across Western Europe and parts of Central Asia from 34,000 years ago until medieval times.
Analysis of this uniquely detailed pool of ancient genetic information suggests genes that may have once protected prehistoric hunter-gatherers or Bronze Age herders from harmful pathogens may today increase the risk of neurodegenerative diseases such as multiple sclerosis and Alzheimer’s in Europeans.
The ambitious five-year project involving a team of 175 international experts combined previously known ancient genomes with freshly sequenced DNA from hundreds of skeletal specimens sourced from museums and other institutions across Europe. Together this data forms the world’s largest ancient gene bank, according to the scientists involved in the project.
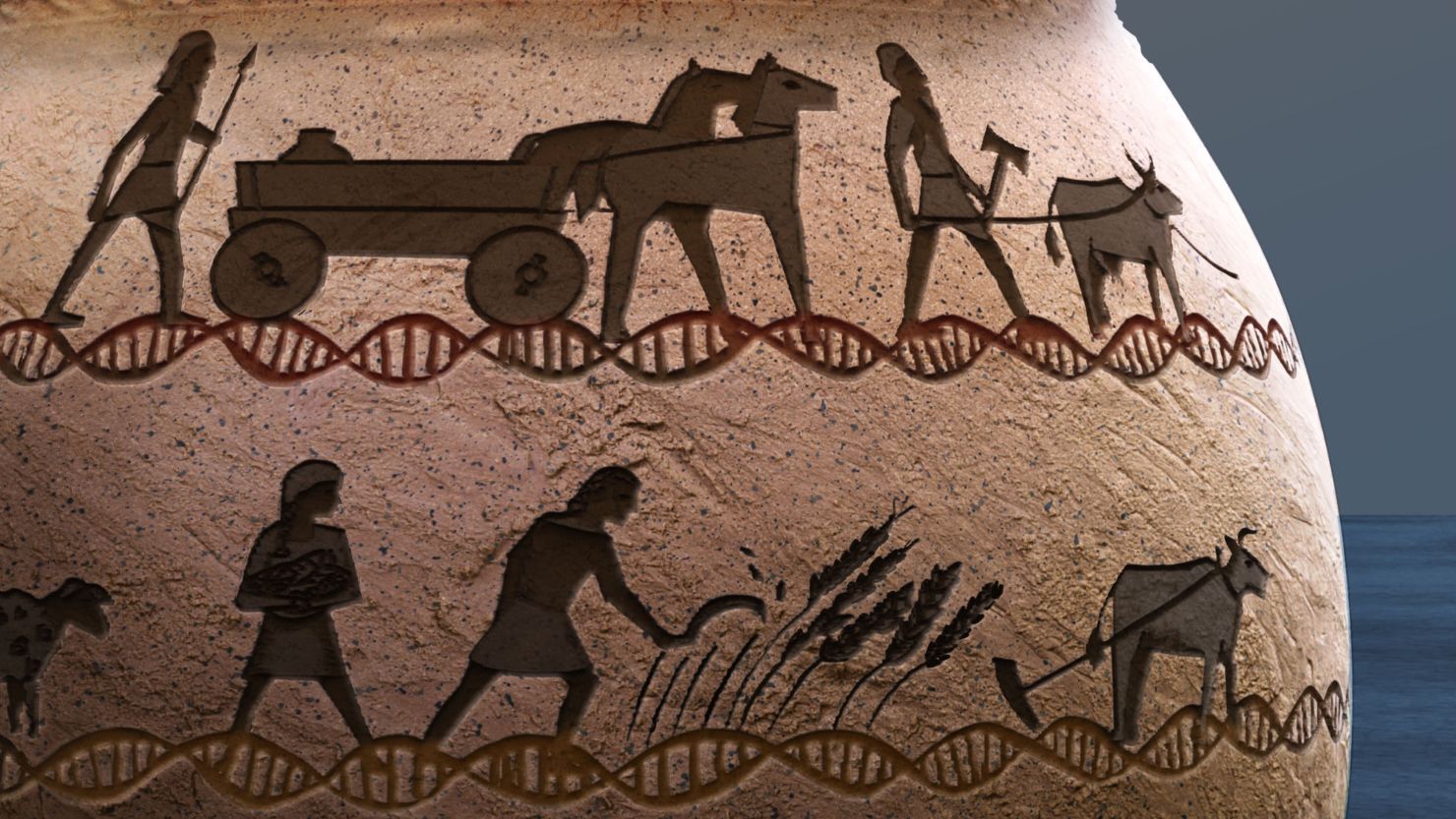
Researchers were able to use the database to chart the spread of genes — and diseases — over time as populations migrated and interbred, revealing how specific and dramatic changes in environment, such as the shift from a hunter-gatherer lifestyle to farming, favored certain genetic variants.
By comparing the ancient DNA with modern-day samples, the researchers gained a new biological understanding of debilitating disorders and physical traits in the present day. The initial results from the project were published in four papers in the scientific journal Nature on Wednesday.
“What’s remarkable about this dataset is that now we can actually see what happened in the past, we can actually see what are the genetic variants that change in frequency in the past due to natural selection. And that allows us this very, very fine-grained picture,” said Rasmus Nielsen, a professor of integrative biology and geneticist at the University of California, Berkeley, who helped spearhead the project, at a news briefing this week.
The researchers sequenced DNA from human remains in museum collections around Europe.The Danish National Museum
How Bronze Age herders are linked to MS
One of the key findings from the first batch of research, based on more than 1,600 genomes in the database, was connected to multiple sclerosis, often called MS, a lifelong autoimmune disease of the nervous system that affects an estimated 2.5 million people worldwide. It’s a complex condition shaped by multiple environmental and genetic factors with many potential symptoms, including problems with vision, arm or leg movement, sensation, and balance.
ADVERTISING
Northern Europeans are among those most prone to the the disease, the study noted, but the reasons why are little understood.
Researchers used the database to explore the genetic origins of multiple sclerosis. They found that genetic risk of having the condition correlates to the proportion of ancestry from a group of ancient pastoralists who introduced domesticated animals to Europe around 5,000 years ago.
These nomadic herders of cattle and sheep, known as the Yamnaya, originated from the Pontic steppe, which stretches from southeastern Europe into Kazakhstan. It’s thought they were the first horse riders, making them highly mobile.
When they moved westward into Europe, they brought specific genetic variants that the researchers believe evolved to protect the nomads against pathogens carried by domesticated animals, the study found.
These genetic variants may have subsequently proved beneficial to European populations in making the shift from hunting and gathering to farming.
And because the Yamnaya primarily moved into northern Europe, the team concluded that the increased proportion of pastoralist ancestry in present-day northern Europeans might be partly responsible for the higher prevalence of the disease there.
“These results astounded us all. They provide a huge leap forward in our understanding of the evolution of MS and other autoimmune diseases,” said William Barrie, a postdoctoral researcher in the University of Cambridge’s department of zoology and coauthor of one of the papers, in a statement. “Showing how the lifestyles of our ancestors impacted modern disease risk just highlights how much we are the recipients of ancient immune systems in a modern world.”
Today, the protective benefits of these genetic variants are no longer as useful, noted coauthor Astrid Iversen, a professor virology and immunology at the University of Oxford.
“We now lead very different lives to those of our ancestors in terms of hygiene, diet, and medical treatment options and this combined with our evolutionary history means we may be more susceptible to certain diseases than our ancestors were, including autoimmune diseases such as MS,” Iversen said in a statement.
Alzheimer’s link
Researchers also mapped the origins of a genetic variant, APOE ε4, known to increase the risk of Alzheimer’s disease. The gene was linked to early hunter-gatherer populations that once inhabited prehistoric Europe, one of the four studies found.
“DNA from hunter-gatherers is present at higher levels in Northeastern Europe, which means the region has an elevated genetic risk of developing Alzheimer’s disease,” Barrie said.
In commentary accompanying the research, Samira Asgari, an assistant professor in genetics and genomic sciences at the Icahn School of Medicine at Mount Sinai in New York, said that it was crucial to extend these types of studies beyond Europe to other regions to “better understand how differences in population history might have contributed to the risk of autoimmune diseases such as multiple sclerosis.”
“Although human biology is shared, each population has a unique history and focusing on a single population limits opportunities for discoveries that can bring insights that advance medicine,” wrote Asgari, who was not involved in the four studies.
The new database provides the “most comprehensive views of the genetic history of a region to date,” said Tony Capra, an associate professor of epidemiology and biostatistics in the Bakar Computational Health Sciences Institute at the University of California, San Francisco.
“This has enabled the authors to fill in missing details in our understanding of both who lived where and when as well as how natural selection shaped the traits of modern individuals,” he said.
However, Capra cautioned that there is “rarely a simple answer to why one population may have a genetic variant while another does not.”
“The evolutionary history of our species makes many contributions to our health and traits today,” said Capra, who wasn’t involved in the research, via email.
“However, both then and now, all these genetic effects are modulated by the environment. And for most traits, MS included, the genetic effects are the result of multiple genetic variants,” he said. “Ultimately, we can’t say that MS came from Bronze Age populations, but these populations’ movements and environments contribute to differences in MS risk today.”
Posted inMost Recent|Comments Off on About MS and Alzheimer’s…..
Ping Suhai is a Qi gong exercise that has a suggestion in it that reminds us to smile. This aspect of Ping Shai alone has had a profound effect on me. When I smile, I can feel my happy life just ahead and I can see it through the fog. Like a puzzle that opens a new skill, Ping Shuai continues to capture me for almost a year now, and the happy life get closer.
Now, something new is happening. I now say to myself, (with a big smile), “I found it”. Then the big smile gets even deeper. This has been happening a lot! I found money, I found more love, I found happiness, I found everything that I wanted for my children, I found easy solutions to that which has been up until now, feeling kind of “hard”. All of these things complete themselves with higher self-esteem. I have stopped telling myself that I am sick/weak/unloveable or any other low self-esteem thing that still has clung to to me from my past. I can easily now step over it and walk away.
“I found it” means to me that I have connected to what I was looking for!!! Strangely, it has been here all along, (like The Wizard of Oz that I watched every year on Thanksgiving). I found it, doesn’t seem to be physical, it is an alignment inside myself. I went from disconnected in some way from life that has been going on for my whole life, to being in it fully in a physical way. This is real and it flows right into the physical world. When I say I found it, or I am about to find it, I go into a state of allowing it to be. It is a peaceful state of being that is satisfying.
This peaceful state, acknowledges that I have been looking for whatever it is that comes up when I say “I found it”. It also completes it. It has some ability to create connection to power than can connect me to what I am looking for. It includes all of its completion. When I am looking for what it is that I look for, perhaps in that peaceful state, I enter into a state of curiosity. But, it is not that I enter or that I am curious or that I am trying to get it with my mind as a symbol of satisfaction. Rather, the state of being allows me to flow there. It is this flow that is spiritual and energetic and can bridge the physical and the energetic. When I find what I have been looking for, it changes everything both inside me, especially in my imagination (as a state of higher consciousness) and on the outer physical world which in the past has been more laborious to achieve.
The Ping Shuai has an important aspect to it that I believe contributes to my body being able to flow in this peaceful state of being that I describe as “all the way well”. It does something that most people miss. It has to do with body fluids mixing and being able to move in the body. It requires exercise and shaking up the body as we are an oil and water emulsion. It is a way of breathing deeply and scanning from the top of the inhaled breath to the bottom of the exhale so the body can see itself in entirety. A great man from England told us in a health seminar that the top of the breath, if it is cut short, can lead to “itis” or infection. If the bottom of the breath scan is cut short, it can lead to an “otis” or cancer. So lately, I have been able to assist my body to eliminate toxins with the most powerful method I have found. Breathing. The presence of Oxygen is the absence of disease. So I watch my breath carefully. The exhale is meant to eliminate toxins from the blood. But I don’t breath if I am working intently unless I train myself. Usually, people who are sick, have very shallow breath strokes. I trained myself 15 years ago with a symbol on the bottom of my computer screen.
I use my breath to move the skin on the bones, the connective tissue and the movement that the glands depend on to balance the hormones and to rebuild the structures of my body that I break down due to bad habits. If I am not happy, I land on my liver. I get angry and whiney inside. This is definitely a neurotransmitter issue which I have corrected over time, but nothing like what has happened since I started using live Natto-kinese in the form fresh mushroom sprouts grown on black beluga lentils. This is a fresh culture process much like Bravo Yogurt. Then I eat a few tablespoons of the lentil-natto with Bravo Yogurt and avocado for breakfast with my supplements. Before that, when I very first wake up, I drink lots of water. I used to push water and force myself to drink it. This was hard on my kidneys. Now, I just drink what my body wants and keep fresh water available in my environment so that that my body gets it when it wants it. In morning meditation, I don’t sit with my back on a chair. Sitting is not good for my body, my kidney tubes, or the fluids which settle too much. At night when I sleep. the fluids are draining and moving and cleaning.
In the 1930. Budwig got the Nobel peace prize for setting up a winning combination for health. A specifically cultured cottage cheese with a vitally alive flax oil. I have a seed press and 50 pounds of fresh seed. Mostly black sesame which has been used for oil pulling for 2000 years. Bravo yogurt is the best I have ever used for Budwig’s cottage cheese. Dr. Steven Gundry’s Moroccan olive oil is one of the best for giving my body Polyphenol-Rich nutrients needed for body smoothness and to keep the oils in the body fresh. Imuno is simply amazing at keeping the power going in the body so that I can lift my energy and not bump along in this world. Many of my customers are people who are high achievers and want more reach!
I am always open to being taught and to provide people with a custom plan to use the products. Feel free to reach out to me on the www.healthyenergetics.com pink chat button. Let me know what you are trying to do and what you have done about so far. and doing me in becoming all the way well.
Look for 30 min session of Ping Shai on YouTube.
🙂
Mimi
Posted inMost Recent|Comments Off on The Benefits of Ping Shuai
García-Aguilar I, Zwaan S, Giomi L. Polymorphism in tubulin assemblies: A mechanical model. Phys Rev Research. 2023;5:023093.
Gardiner J. Insights into plant consciousness from neuroscience, physics and mathematics: a role for quasicrystals? Plant Signal Behav. 2012;7(9):1049–1055.
Hameroff S. ‘Orch OR’ is the most complete, and most easily falsifiable theory of consciousness. Cogn Neurosci. 2021;12(2):74–76.
Hameroff S, Penrose R. Consciousness in the universe: a review of the ‘Orch OR’ theory. Phys Life Rev. 2014;11(1):39–78.
Hameroff S. ‘Smear campaign’ at the crossroad of consciousness and spacetime geometry -: Comment on “At the crossroad of the search for spontaneous radiation and the Orch OR consciousness theory” by Derakhshani et al. Phys Life Rev. 2023;44:173–175.
Ichikawa M, Bui KH. Microtubule inner proteins: a meshwork of luminal proteins stabilizing the doublet microtubule. Bioessays. 2018;40(3).
Lamme VAF. Challenges for theories of consciousness: seeing or knowing, the missing ingredient and how to deal with panpsychism. Philos Trans R Soc Lond B Biol Sci. 2018;373(1755):20170344.
Reddy JSK, Pereira C. Understanding the emergence of microbial consciousness: From a perspective of the Subject-Object Model (SOM). J Integr Neurosci. 2017;16(s1):S27–S36.
Ruggiero M (a). Study of structural similarities between tubulin, TMC1, AND FTSZ proteins as they relate to mechanosensory transduction in the context of the orch or theory of consciousness. Int J Radiol Radiat Ther. 2023;10(3):65‒72.
Ruggiero M (b). On the Natural intelligence and consciousness of the immune system and its relationship with the brain. Preprints. 2023:2023081335.
Ogryzko VV. Erwin Schroedinger, Francis crick and epigenetic stability. Biol Direct. 2008;3:15.
Peris L Thery M, Fauré J Saoudi Y, Lafanechère L, et al. Tubulin tyrosination is a major factor affecting the recruitment of CAP-Gly proteins at microtubule plus ends. J Cell Biol. 2006;174(6):839–849.
Hameroff S. Consciousness, cognition and the neuronal cytoskeleton
a new paradigm needed in neuroscience. Front Mol Neurosci. 2022;15:869935.
Pavlov CS, Damulin IV, Shulpekova YO, et al. Neurological disorders in vitamin B12 deficiency. Ter Arkh. 2019;91(4):122–129.
Wu F, Xu K, Liu L, et al. Vitamin B12 enhances nerve repair and improves functional recovery after traumatic brain injury by inhibiting er stress- induced neuron injury. Front Pharmacol. 2019;10:406.
Sangle P, Sandhu O, Aftab Z, et al. Vitamin B12 supplementation: preventing onset and improving prognosis of depression. Cureus. 2020;12(10):e11169.
Shipton MJ, Thachil J. Vitamin B12 deficiency – A 21st century perspective. Clin Med (Lond). 2015;15(2):145–150.
Li S, Guo Y, Men J. et al. The preventive efficacy of vitamin B supplements on the cognitive decline of elderly adults: a systematic review and meta-analysis. BMC Geriatr. 2021;21:367.
Miller A, Korem M, Almog R, et al. Vitamin B12, demyelination, remyelination and repair in multiple sclerosis. J Neurol Sci. 2005;233(1- 2):93–97.
Lauer AA, Grimm HS, Apel B, et al. Mechanistic link between vitamin b12 and alzheimer’s disease. Biomolecules. 2022;12(1):129.
Dietiker C, Kim S, Zhang Y, et al. Characterization of vitamin b12 supplementation and correlation with clinical outcomes in a large longitudinal study of early parkinson’s disease. J Mov Disord. 2019;12(2):91–96.
Arnon R, Aharoni R. Mechanism of action of glatiramer acetate in multiple sclerosis and its potential for the development of new applications. Proc Natl Acad Sci U S A. 2004;101 Suppl 2(Suppl 2):14593–14598.
Kopf A, Kiermaier E. Dynamic microtubule arrays in leukocytes and their role in cell migration and immune synapse formation. Front Cell Dev Biol. 2021;9:635511.
Frederickson CJ, Suh SW, Silva D, et al. Importance of zinc in the central nervous system: the zinc-containing neuron. J Nutr. 2000;130(5S Suppl):1471S–1483S.
Drewes G, Lichtenberg-Kraag B, Döring F, et al. Mitogen activated protein (MAP) kinase transforms tau protein into an Alzheimer-like state. EMBO J. 1992;11(6):2131–2138.
Hesketh JE. Zinc-stimulated microtubule assembly and evidence for zinc binding to tubulin. Int J Biochem. 1982;14(11):983–990.
Gower-Winter SD, Levenson CW. Zinc in the central nervous system: from molecules to behavior. Biofactors. 2012;38(3):186–193.
Li Z, Liu Y, Wei R, et al. The important role of zinc in neurological diseases. Biomolecules. 2022;13(1):28.
Wang FD, Zhao FJ, Jing NH. Effect of dietary zinc on microtubule- associated protein 2 expression in the brain of mice]. Sheng Li Xue Bao. 1999;51(5):495–500.
Sikora J, Ouagazzal AM. Synaptic Zinc: An emerging player in parkinson’s disease. Int J Mol Sci. 2021;22(9):4724.
Abdel-Latif HMR, Dawood MAO, Alagawany M, et al. Health benefits and potential applications of fucoidan (FCD) extracted from brown seaweeds in aquaculture: An updated review. Fish Shellfish Immunol. 2022;122:115–130.
Atashrazm F, Lowenthal RM, Woods GM, et al. Fucoidan and cancer: a multifunctional molecule with anti-tumor potential. Mar Drugs. 2015;13(4):2327–2346.
Apostolova E, Lukova P, Baldzhieva A, et al. Immunomodulatory and anti-inflammatory effects of fucoidan: a review. Polymers (Basel). 2020;12(10):2338.
Husni A, Izmi N, Ayunani FZ, et al. Characteristics and antioxidant activity of fucoidan from sargassum hystrix: effect of extraction method. Int J Food Sci. 2022;2022:3689724.
Bakunina I, Chadova O, Malyarenko O, et al. The effect of fucoidan from the brown alga fucus evanescence on the activity of α-n- acetylgalactosaminidase of human colon carcinoma cells. Mar Drugs. 2018;16(5):155.
Krylova NV, Ermakova SP, Lavrov VF, et al. The comparative analysis of antiviral activity of native and modified fucoidans from brown algae fucus evanescens in vitro and in vivo. Mar Drugs. 2020;18(4):224.
Kwon PS, Oh H, Kwon SJ, et al. Sulfated polysaccharides effectively inhibit SARS-CoV-2 in vitro. Cell Discov. 2020;6(1):50.
Pradhan B, Nayak R, Patra S, et al. A state-of-the-art review on fucoidan as an antiviral agent to combat viral infections. Carbohydr Polym. 2022;291:119551.
Ushakova NA, Morozevich GE, Ustiuzhanina NE, et al. Anticoagulant activity of fucoidans from brown algae. Biomed Khim. 2008;54(5):597– 606.
Li J, Chen K, Li S, et al. Protective effect of fucoidan from fucus vesiculosus on liver fibrosis via the tgf-β1/smad pathway-mediated inhibition of extracellular matrix and autophagy. Drug Des Devel Ther. 2016;10:619–630.
Roberts M. Capitalism, psychiatry, and schizophrenia: a critical introduction to deleuze and guattari’s anti-oedipus. Nurs Philos. 2007;8(2):114–127.
Ruggiero M The Human microbiota and the immune system; reflections on immortality. Madridge J Immunol. 2017;1(1):18–22.
Ruggiero M The brain microbiota as it relates to the orch or theory of consciousness. J Neurol Stroke. 2021;11(5):131‒133.
Farmer JD, Packard NH, Perelson AS. The immune system, adaptation, and machine learning. Physica D: Nonlinear Phenomena. 1986;Vol 22(1–3):187–204.
Posted inMost Recent|Comments Off on Design and development of novel compounds aimedat optimizing the function of microtubules andtubulin in the immune system and the brain
When Bravo Yogurt began over 10 years ago, the starter powders were all made in Switzerland. But in 2016, the FDA had a chat with Dr. Ruggiero about being able to sell it in the USA and wanted FDA approved colostrum. Thus, they got FDA approved colostrum and the people of the USA rejoiced to have Bravo!
Now, the yodeling cows are back! The colostrum is now 100% Swiss and organic from certified suppliers and strictly tested of course.
The colostrum will be more yellow and a bit more oily than before due to the ingredients changing their source. Assurances of its performance were given!
Correspondence: Marco Ruggiero, MD, PhD, National Coalition of Independent Scholars , 125 Putney Rd, Battleboro, VT 05301, USA
Received: June 25, 2021 | Published: September 8, 2021
Citation: Ruggiero M. The brain microbiota as it relates to the orch or theory of consciousness. J Neurol Stroke. 2021;11(5):131-133. DOI: 10.15406/jnsk.2021.11.00471
It is proposed to incorporate the concepts of brain microbiota and microbial consciousness in the Orchestrated Objective Reduction (Orch OR) theory of human consciousness with the goal of increasing its explanatory and predictive powers. If consciousness arises from quantum computations in cytoskeletal structures inside human neurons, there is no theoretical impediment at hypothesizing that it might also occur in the cytoskeletal structures of the microbes resident in the human brains. If the concept of the brain microbiota is integrated in a general Orch OR theory, its explanatory and predictive powers would be vastly increased.
A recent article by Hameroff describes Orchestrated Objective Reduction (Orch OR) as “the most complete, and most easily falsifiable theory of consciousness”.1 The Author proposes an experiment, based on exposure to anesthetic gases, that would confirm or reject the theory that consciousness is based on quantum computations occurring inside microtubules of brain neurons rather than in the plasticity of the web of connections established between cells of the central nervous system as proposed by the majority of theories of consciousness.2
The basic tenets of the Orch OR theory of consciousness
Orch OR is a revolutionary theory of consciousness published by Nobel Laureate Sir Roger Penrose and Professor Stuart Hameroff for the first time in the mid-nineties,3 and further elaborated in successive publications.1 A common denominator of the various evolutions and revisions of the theory is the concept that consciousness has its origin inside brain neurons, thanks to phenomena of quantum computing that occur in the context of subcellular structures, the microtubules, and involve the conformational arrangement of a protein, tubulin. This theory is fundamentally different from all other theories of consciousness that postulate the origin of consciousness in the web of synaptic connections between neurons. According to the Orch OR theory, consciousness is the result of a sequence of discrete phenomena, each being an instant of OR of a quantum state, where it is postulated that these quantum states are present as components of a biological quantum computing machinery operating inside the conformation of the protein molecular structure of neuronal microtubules. Actual consciousness is self-generated when these phenomena of OR are “orchestrated” in an adequate manner. Orchestration occurs thanks to inputs from other neurons through wireless transmission of resonant vibrations, quantum entanglement or classic synaptic transmission as well as to inputs arising inside the microtubules that constitute a sort of memory. Given the quantum nature of the computation events, these can be transmitted to a significant number of neurons across wide areas thus generating a quantum activity of large scale inside the brain. A point that differentiates the Orch OR theory from all other theories of consciousness is that its implications are not limited to neuroscience or biochemistry, but extend to general relativity and quantum physics with ramifications in the fields of philosophy and spirituality. A most intriguing aspect of the theory consists in the implication that the processes of quantum computing due to Orch OR, as they occur in neuronal microtubules, are intimately connected with the processes operating at the level of the fine structure of the universe. Minute perturbations of the space-time fabric at the Planck/quantum level are deemed to be responsible for OR both in the brain and in the universe. In other words, the OR events that are responsible for computing and generation of consciousness when orchestrated, are the same that are at work at the level of the basic structure of the universe where minute perturbations of quantum coherence of the space-time fabric are considered responsible for the OR or the collapse to just one single state as originally postulated by Penrose.4 In this interpretation, the Orch OR theory connects the working of the brain with that of the universe. In the decades after its inception, the theory has received many constructive criticisms that led to evolutions and revisions of the original theory, whose chore tenets, however, have never been proven false. Actually, as per the classical Falsification Principle by Popper, its falsifiability makes the theory stronger than many others up to the point that Hameroff entitled his latest article ‘Orch OR’ is the most complete, and most easily falsifiable theory of consciousness.4 In order to demonstrate the completeness and easy falsifiability of the theory, Hameroff proposes four paradigm cases:
Conscious vs non-conscious states; is the theory able to distinguish between the two states?
Small network criterion; how many neurons are necessary for consciousness to arise?
Reduced brain volume; there are people with significantly reduced brain volume, practically with no brain.5 How can consciousness arise if not through Orch OR?
Minimization of mysteries; the Occam’s razor favors minimization of mysteries, thus favoring the hypothesis that Orch OR has explanatory value for a number of mysteries ranging from neuroscience to general relativity and quantum physics.1 (Hameroff, 2021).
Here, it is introduced a fifth paradigm case that should be taken into consideration in designing experiments aimed at falsifying the Orch OR as well as any other theory of consciousness.
The fifth paradigm, the brain microbiota
Hameroff and all those concerned with theories of consciousness focus their attention on the human cells of the brain, neurons and glial cells, but do not take into account the presence of microbial cells that constitute the brain microbiota, whose influence on brain function is nothing less than “immense”.6 The first description of bacterial cells in the brains of healthy individuals was published in 2013;6 the term “brain microbiota” in the context of neurological diseases was used for the first time in 2016.7 In 2018, ultrastructural studies demonstrated abundance of microbial cells in the areas associated with reward-seeking, learning, memory and consciousness, i.e. the substantia nigra, the hippocampus and the pre-frontal cortex.8 The microbes in human brains are the same that are found in soil and water; it has been hypothesized that they reach the brain carried by cells of the immune system as well as travelling along the axons of peripheral nerves.6,8 Whatever the case, just as it would be unrealistic today to discuss the function of the gut, or that of the immune system, without considering the essential role of the microbiota,9 it is proposed that also the discussion on the different theories of consciousness, and, in particular, Orch OR, should take into account the role of the brain microbiota.
Microbial consciousness
If consciousness arises from quantum computations occurring in cytoskeletal structures inside human neurons, there is no theoretical impediment at hypothesizing that cytoskeletal structures of microbes could give rise to forms of consciousness or awareness. Microbial consciousness arising from the cytoskeleton was described in 201710 and this concept was further elaborated in an essay published in 2019 where the Authors postulate that subjective awareness emerged as an intrinsic feature of the first unicellular forms of life through the working of oscillating cytoskeletal structures, and structurally flexible proteins, that is, in a manner closely reminiscent to the concepts at the basis of Orch OR.11 If phenomena of quantum entanglement occur between the microtubules of adjacent neurons,12 they will also occur between the cytoskeletal structures of human neurons and those of the microbes of the brain microbiota as well as between the cytoskeletal structures of the different microbes. Wireless and quantum entanglement-based communication between microtubules of individual neurons has been theoretically conceived and experimentally demonstrated,13 thus supporting the hypothesis that the process of orchestration can take place on a large scale, in theory involving all neurons across the wholeness of the brain. According to what is proposed here, these phenomena of communication are not restricted to human neurons, but are extended to the brain microbiota. This is all the more conceivable when considering that wireless communication based on the resonance of vibrations inside microtubules does not require neurotransmitters or synapses14 and, therefore, can occur between neurons and microbial cells even though they are not anatomically connected by synapses. It is worth noticing that the interpretation of Orch OR described here is consistent with the concepts put forward by Barlow15 who described how the Orch OR theory can explain consciousness of plants.
Implications for the design of experiments
In designing an experiment to prove Orch OR, Hameroff proposes to expose the brain to anesthetic gases and observe whether dampening of quantum interference beats in tubulin and microtubules occurs.1 However, volatile anesthetics affect bacterial functions such as motility, biofilm formation and signal transduction. Of particular significance are the effects on biofilm formation since this phenomenon is paradigmatic of the so-called microbial intelligence.17 In short, in designing the experiment to prove or falsify Orch OR, the effects of volatile anesthetics on the brain microbiota should be considered in order to prevent potential misinterpretation of the results.
Conclusion
Orch OR might indeed be the most complete theory of consciousness even though it has to be considered special or relative to the human part of the brain; if the concept of the brain microbiota and the ensuing concept of the rhizome18could be integrated in a more general Orch OR theory, its explanatory and predictive powers would be vastly increased. For example, the Orch OR theory postulates that consciousness may exist independently of biological substrates, namely human neurons.13The cases of people with vastly reduced brains who lead normal lives appear to support this postulate.5If the concept of the microbiota is incorporated in the Orch OR theory, the issue of permanence of consciousness independently of neurons would be further supported by the consideration that the microbiota survives the human body;18 if the Orch OR phenomena occurring inside the microtubules of human neurons are entangled and shared with the microbiota, an organ that has 10 times more cells and 100 times more DNA-based information than its human counterparts in our bodies, then survival of consciousness becomes a microbiological rather than a philosophical issue.
Acknowledgments
The Author wishes to thank the staff at Silver Spring, Switzerland, for inspiring discussion.
Roberts RC, Farmer CB, Walker CK. The human brain microbiome; there are bacteria in our brains! 594.08/YY23. Session 594. Neuroscience. 2018. Neuroimmunology: Regulating Systems. 2018.
If you have been diagnosed with cancer, or have a loved one that is suffering from cancer, chances are you have heard about the Joe Tippens Cancer Protocol. The Fenbendazole Cancer Protocol has been gaining rapid interest over the past years following some fenbendazole advanced cancer success stories.
Joe Tippens founded the protocol after he was told a story about a scientist at Merck Animal Health that had been performing cancer research on mice. The research included injecting different types of cancers into different mice body parts. The scientists discovered, through trial and error, a product in their canine product line, fenbendazole, that was batting 1.000 in killing these different cancers in the mice. The scientist was later diagnosed with stage 4 brain cancer and was given a grim prognosis of only three months to live. She decided to try the fenbendazole, and after six weeks, showed a clean scan.
Joe Tippens had been initially diagnosed with small cell lung cancer. The cancer later spread to his neck, right lung, stomach, liver, bladder, pancreas and tail bone. Like the scientist from Merk Animal Hospital, Joe was told he only had three months to live. In 2017, after hearing the story of the scientist who treated her cancer with a canine drug, Joe decided he was going to do the same. However, in addition to taking the fenbendazole, Joe added his own ingredients to the regimen (curcumin, CBD oil, and vitamin E), thus creating the Joe Tippens Cancer Protocol.
Disclaimer: We in no way endorse the Joe Tippens Cancer Protocol as a cure for cancer, and as always, you should consult your physician before starting any new medications or treatment plans.
What Is Fenbendazole?
According to Wikipedia, Fenbendazole is a broad spectrum anthelmintic used against gastrointestinal parasites including: giardia, roundworms, hookworms, whipworms, the tapeworm genus Taenia (but not effective against Dipylidium caninum, a common dog tapeworm), pinworms, aelurostrongylus, paragonimiasis, strongyles, and strongyloides that can be administered to sheep, cattle, horses, fish, dogs, cats, rabbits, most reptiles, freshwater shrimp tanks as planaria and hydra treatments, as well as seals.
Common brand names include Pancur, Panacur C and Safe-Guard.
However, it is also being used by humans in a cancer treatment method known as the Joe Tippens Protocol.
Is fenbendazole a cancer cure scam? One study suggests that fenbendazole has “been safely utilized as an anti-parasitic for various different animal species and could be repurposed for treating human malignancies.” Other benzimidazoles, including albendazole, parbendazole, mebendazole and flubendazole have already been shown to have promising results in humans.
Another study states that the “repurposing of veterinary drugs showing promising results for human use can result in considerable time and cost reduction required to develop new drugs.”
Fenbendazole Protocol – A Simple Step-by-Step Guide
The basic fenbendazole protocol people follow is surprisingly simple and includes a few added supplements to the fenbendazole:
** Mimi does not recommend CBD oil. It will scar the subtle energy bodies.
Fenbendazole which has 222mg of Fenbendazole per gram: one packet of powder per day for seven days a week. It can be mixed with food such as yogurt or simply taken by itself.
2. Curcumin: 600 mg a Day
600 mg per day of bioavailable curcumin, which is the active agent in the herb turmeric. Curcumin may help increase healthy p53 levels, and it has been shown to be a potentially effective cancer therapy supplement.
** Mimi does not recommend CBD oil. It will scar the subtle energy bodies.
25 milligrams daily, taken sublingually (under the tongue). The CBD oil should be high-purity level broad-spectrum. CBD has been shown to potentially modulate tumor growth.
To enhance CBD healing response for cancer symptoms, slowly increase to 0.5ml of CBD twice daily for a total of 50 mg.
4. Berberine: 2-3 times a day
Berberine has shown important anti-tumor effects in numerous studies. These studies reported that Berberine could prevent the multiplication of cancer cells and inhibit metastasis and the spread of cancer cells. Berberine can work with Fenbendazole to further limit the cancer cells’ ability to take up glucose. This way, cancer cells are weakened and starved.
Due to its antioxidant, anti-tumor, and anti-inflammatory activities, quercetin has been studied extensively. Quercetin can inhibit the spread of many cancers such as prostate, cervical, lung, breast, and colon. Quercetin is not harmful to healthy cells yet powerful against cancer cells, making it a good candidate for a supplementary factor along with other anticancer medications.
Can fenbendazole be taken in tablet, liquid or powder?
Fenbendazole is available in tablets (Happy Healing Store), liquid (Safeguard) and powder (Panacur). There may be other formulations available, but those are the primary products that patients are using.
Is it safe for humans to take fenbendazole?
Since fenbendazole is a veterinary medicine, and is not licensed for human use and there is no specific human safety data available. The similar human forms of this class of medications, mebendazole and albendazole, have been used for parasitic infections for many years and have a good safety record. Fenbendazole has been reported to have a very low degree of toxicity and a high degree of safety in animal experiments.
Is fenbendazole toxic for the liver?
Although fenbendazole is generally well tolerated, there have been reports of elevated liver enzymes from the use of fenbendazole, as well as the human medications mebendazole and albendazole.
I’ve found a Fenbendazole brand which is not made by Merck, is it ok?
There are a variety of opinions on which product is best, but no research exists that compares the effectiveness of various formulations in humans. Merck and Safeguard are well established companies whose products have been safety tested in animals and used by veterinarians for many years.
Would the fenbendazole protocol work with conventional treatment? – chemotherapy?
Yes, fenbendazole has the potential to synergize with conventional treatments, and possibly enhance treatment response. Some aspects of the protocol, such as vitamin E and curcumin, may interfere with chemotherapy and radiation due to their anti-oxidant properties.
Some people take it 3 day on 4 off, some 1 gram a day, some 2 or even 4 grams a day. What is the correct dosage?
Joe Tippens, who popularized the use of Fenbendazole for cancer, recommends 222 mg for three consecutive days, then four days off. There are many people who take larger doses, more frequently. Since Fenbendazole is not licensed for the treatment of cancer in humans, there is no correct dose that is supported by research, pharmacists or physicians. The dose you choose to take should be assessed based on your other medications and treatments, your type of cancer, prognosis, organ function and lab values.
How long do I need to be on this protocol?
This will be up to you based on your treatment response to the protocol. It is reported that Joe Tippens continues to use the protocol for prevention.
How do I know when it is time to dose up?
This is an individual decision based on treatment response, tolerance, other treatments/medications and lab values.
<div class=”player-unavailable”><h1 class=”message”>An error occurred.</h1><div class=”submessage”><a href=”https://www.youtube.com/watch?v=mnAX1-K81oQ” target=”_blank”>Try watching this video on www.youtube.com</a>, or enable JavaScript if it is disabled in your browser.</div></div>
What’s Joe Tippens doing in 2022 to stay cancer free?
One of the contributors from CancerDefeated.com met Joe in person and interviewed him in April 2022. Here’s what she discovered…
Joe’s scan was completely clear in early 2017. His scan in Feb. 2022 still shows no evidence of disease.
Since cancer is notorious for recurrences, Joe continues to follow his regimen for prevention… and plans to for the rest of his life. However, he recently revamped the rest of his entire cancer treatment protocol.
Joe has scaled back to three days a week on the FenBen, now that he’s been cancer-free for five years. He recommends staying on the seven-day fenbendazole protocol till you’re cancer-free for at least three years.
Based on his extensive research, he’s added things to his protocol. including Frankincense and berberine. All products are in a much more bioavailable form, too. He notes that getting absorption of nutrients into the bloodstream is a bigger problem than most people realize. His new protocol helps address this problem.
Joe spent much of 2021 collaborating with scientists and M.D.’s in the pharmaceutical and nutraceutical space, to develop processes that dramatically improve nutrient delivery into the bloodstream at previously unheard-of levels.
Here’s the three-pronged approach he uses in 2022 (R):
1: Support healthy cell division. Joe consumes cryogenically extracted CEM™ Hemp. Getting the terpenes and cannabinoids from full-spectrum hemp is critical to gaining its best benefits. The product is now cryo-extracted to preserve these substances. It also includes Frankincense and a Nano MCT oil.
2: Support healthy cell life cycles and clearance of dead cells with curcumin. Curcumin was always part of Joe’s protocol. He previously used the most bioavailable curcumin product he could find. He cringes when he relates how much he was depending on a nutrient that’s so
Reversing Chronic Kidney Disease with Niacin and Sodium Bicarbonate
By Stephen McConnell and W. Todd Penberthy Orthomolecular Medicine News Service
This story began with initial discovery, motivated by necessity. It would lead a few years later to reproducible documented reversal of chronic kidney disease (CKD) stages 1 or 2. Success was achieved using 3 to 5 cents/day of 100-500 mg niacin TID [three times a day] along with 1.0-1.8 grams of sodium bicarbonate (baking soda, 600 mg at lunch and 1.2 g before bed) with or without <2g/day elemental calcium, as calcium carbonate.
Excellent results from the use of niacin to treat CKD have now been documented for more than 25 case-studies. This approach is well supported by continuous basic and clinical research, including dozens of clinical trials that provide substantial evidence for the use of niacin and sodium bicarbonate. These approaches directly address the needs of the typical CKD patient. Unfortunately, this approach is rarely implemented in the clinical setting.
CKD commonly progresses with age as it is observed in 68% of Americans ≥60 years of age.1 Patients with CKD usually experience progressive loss of kidney function moving towards an increasing risk of end-stage renal disease (ESRD). CKD is the 9th leading cause of death in the US.2 Fortunately, there are several simple approaches including the addition of modest doses of niacin (immediate release- or IR-Niacin) that can reverse CKD in many patients as described here.
Approximately 786,000 people per year, in the US progress to ESRD (stage 5 CKD), which is generally considered an irreversible condition. Most of these become completely dependent on regular trips to dialysis. Estimation of the stages of CKD is based on (GFR) glomerular filtration rates starting with ≤60mL/1.7m2 for three months as definitive of initial CKD diagnosis. Unfortunately, a creatinine derived GFR (crGFR) is only as reliable as the serum creatinine measure. Use of this creatinine-based test has a “blind-area” in the earlier stages and frequently leads to an under-estimation of the true risk.
Stages of CKD
Mild kidney damage, eGFR 90 or higher
Mild loss of kidney function, eGFR 60-89
Moderate loss of kidney function a. eGFR 45-59 b. eGFR 30-44
Severe loss of kidney function, eGFR 15-29
Kidney failure or close to failure, eGFR less than 15
Niacin for CKD
Supplementation with daily low-dose niacin reliably reverses a large amount of the functional loss. This simple treatment is effective and critically important. Mortality rates with CKD are striking, as the five-year survival rate for patients doing long-term dialysis is 35% compared to 25% in those with diabetes [T2DM] in the USA.3
Routinely, the first treatment approaches utilized for CKD patients, in the later stages, generally targets control of dysglycemia and reduction of hyperphosphatemia according to KDIGO guidelines.4 Fortunately, there is an ever-increasing abundance of data revealing that simple niacin treatment is a profoundly effective treatment for reducing hyperphosphatemia—and that is just the beginning. In basic research the evidence in favor of niacin for CKD has continuously accumulated. Clinical research proves that the niacin stimulated pathways involving increased NAD synthesis, PCSK9 inhibition, sodium transporter effects, PPAR gamma activation, and more, are exceptionally well-suited to addressing CKD, multimorbidity, and ultimately all-cause mortality.5-41
The clinical and financial impact of CKD when it progresses to end-stage renal disease (dialysis-dependence; ESRD) is profound. Clinically, CKD progression quickly leads to lifelong dialysis with co-morbid life-threatening cardiovascular disease. Financially, the out-of-pocket cost of CKD is greater than cancer and stroke with ESRD dialysis costing 30.9 billion per year in 2013 or approximately 7.1% of total Medicare costs.42Medicare spends approximately $250,000/y for every CKD patient, prior to the transition to ESRD and dialysis. Annual costs per dialysis patient can range from $720k to $2.2m per year.43 These problems and their associated costs can be reduced by using 5 cents per day of niacin.
Originally, I (SM) was formally trained to operate a heart-lung machine, maintain full life-support and anesthesia, in the operating room monitoring patients undergoing open-heart surgery. Much later, I transitioned to working as a field scientist, MSL (Medical Science Liaison) in the advanced laboratory diagnostics industry. My primary clinical focus since that time has mainly been lipidology. Because of my initial education/training, addressing cardiovascular disease, I now focus on prevention: lipidology. This training gave me an appreciation for nicotinic acid (niacin, vitamin B3).
I have now personally observed more than 25 documented cases of individuals having their CKD progression not only halted but reversed with the addition of 3 to 5 cents worth of niacin, per day (with 1.8-2.4 g/day sodium-bicarbonate with/without 250-500 mg/day calcium-carbonate).
A Family Story
While I (SM) was learning lipidology in the period between 2002-2007, my father suddenly went to the ER late one Sunday night and my mother called me hysterically, “I took your father to the ER and now they are scheduling him for placement of stents.” I was concerned, as any son would be, but also as a scientist because I felt I may have ‘failed him,’ somehow: If only what I had already learned, I had only learned it, sooner.
My father was 81 at the time and he had been jumping rope for 30-minutes, twice daily. His body had a deceptively healthy look, and his triglycerides were low, but when we put it all together, he was “Pattern-B”—insulin resistant. He had always been a ‘stodgy,’ stubborn, stoic World War II veteran. He was very introverted and typically had a limited range of emotions: rage, laughter, and silence. Later, I would find out he had Asperger’s.
When I received the advanced laboratory data, it showed that he had low HDL2 and high ApoB. This is far more specific and confers much greater risk vs. an elevated LDL-C. Most importantly, this revealed he was insulin resistant (a.k.a. pre-diabetic). At the time, I really didn’t fully understand this. Even today, most clinicians really do not, due to continued reliance on using only tests for FBG and HbA1c. Ultimately, my father survived, and we continued to institute aggressive medical management: A hard lesson learned.
My father and my mother traveled everywhere together. They commuted, seasonally to Florida each winter, to escape the cold weather in Northwest Pennsylvania. On New Year’s Day, about six months after his MI and stent-placement procedure, I received a call from my mother, “Your father is in the hospital! They’re going to have to do open heart surgery!”
They needed to do an aortic-annuloplasty (aortic heart valve repair), in addition to a quintuple CABG (5 bypass grafts). I thought to myself, “this is getting worse and worse.” Having had previous personal experience working with thoracic surgeons during open-heart operations, I didn’t want the procedure to begin until my brother and I were able to be present. Fortunately, the young thoracic surgeon and the techniques planned were excellent.
Later, in the spring, they returned home to Erie, Pennsylvania, for the follow-up visit. Dr. Dave (the physician who asked me to set-up my 1st lipid clinic) said, “Hey I got some bad news for you. Your dad has renal insufficiency.” I said, “Oh my God, he’s in renal failure, what stage is he?” He did not know. That was a flag. Most clinicians don’t know what stage their CKD patients are because the lab doesn’t do calculations and the creatinine measure is not reliable or accurate. The creatinine measure has very little accuracy until after the CKD has ‘hit’ stage 3B, and beyond.44,45 So, a lot of these patients along the CKD disease continuum, through each progressive stage, appearing to have less risk vs. the ‘true’ risk that is present. It’s better to test a urine sample and see how much protein is recovered and run a Cystatin-C and a crGFR to calculate a more accurate value. At that time, I only knew he was in failure; but when I did the crGFR calculation, I could see that he was well into the latter portion, of CKD-stage 4.
Recently, I had been putting together a new treatment algorithm with substantial literature support, data, on CKD. I was lucky to have been mentored by Dr. William F. Finn.46 Even if a patient has not already been scheduled for dialysis, he explained, and especially if they are currently on dialysis, you must get the serum phosphorus down. Excessive phosphorous is toxic to the kidneys as well as virtually every organ system and the entire body.47,48 Phosphorus is a primary initiator of vascular calcification, among several other pathologies. If the kidneys start to lose a certain fraction of their normal function, the body can no longer efficiently clear phosphorous. When phosphorous serum levels reach abnormal levels, then you begin to saturate the tissues. Then phosphorous binds to calcium and it’s the phosphorous, not the calcium that starts the pathology leading to calcium phosphate stones.
Niacin Helps to Get the Phosphorous Down
Even after you bring serum phosphate down you still have it in the tissues. The only biomarker available in a clinical setting, Fibroblast Growth Factor-23 (FGF-23), reflects the pathology behind long-term exposure to elevated phosphorus. FGF-23 can be decreased, simply by administering niacin.14However, the sodium phosphorous transporter works through a feedback mechanism to make more receptors to compensate.
So, calcium carbonate (from an antacid tablet) is commonly used first to bind the readily available intestinal phosphorous. This is among the cheapest and most effective phosphorus chelator approaches. Calcium carbonate should not be used above 2g/day elemental calcium, which is 40% of most of the formulations: Total 5g/day as calcium-carbonate. This should be administered at mealtime. The idea is to ‘treat the meal’, as there is generally very little phosphorous available to bind, outside of mealtime. When the kidney is in ‘failure’, after meals, excess phosphorous remains uncleared and leads to deposition in the tissues: valve leaflets; at the endothelial barrier; arterial subendothelial space (Mönckeberg’s medial calcification: arteriosclerosis).49 When sodium bicarbonate (baking soda) is administered, based on the landmark study,50,51 the transition from stages-3 & 4 to Stage-5/ESRD/Dialysis, can be reduced by ~80%, with just 1.8 grams sodium bicarbonate, alone. Mealtime dosing BID, (1X 600 mg at lunch and 2X 600 mg at dinner each day, i.e 1.8 g total per day), optimizes the therapy.
In that study, the fraction of people that went to dialysis by the end of two years was roughly 35% on placebo, but the fraction that went to dialysis with the modest dose of sodium bicarbonate, was reduced roughly >80%.50 However, the concerns about sodium intake are frequently expressed. The literature is quite clear on this. The chloride salt of sodium is the issue, not the bicarbonate salt of sodium. This is a key point. We just need to do a better job of identifying them early on. Do not assume the patient is stage 1 or 2 if the creatinine indicated that. We need better, more reliable biomarkers (EXAMP: Cystatin-C) and should insist the insurance companies reimburse for it.
This approach worked amazingly well for my father because he reversed his CKD, by more than two stages! I calculated it incrementally based on where he was at each stage. He was nearing end-stage renal disease (stage 5) and he reverted back to stage 2, which was a virtual miracle at that time! I had never heard of or seen anything similar.
Niacin interested me when I came across a company that was working on a new chelator for phosphorus. I had already seen some literature on an extended-release niacin (ER-niacin) study showing a phosphorus-lowering effect and IR-Niacin having an antiproteinuric effect. Niacin was so effective that it moved the GFR up enough to reverse the baseline status by a full stage, even at very low doses. This seemed to be the plausible explanation for this net result.
Niacin (as well as no-flush niacinamide/nicotinamide) inhibits the sodium phosphate transporter. There are at least twenty peer-reviewed publications demonstrating this.5-41,52-59 What was discovered was, if you want to control phosphorus, niacin is one the most effective methods and its efficacy is not affected by timing relative to meals. As little as 100 mg of niacin will effectively reduce the serum phosphorus.
Some studies refer to this niacin-mediated effect as the “phosphorous fix.” The additional CKD benefits of niacin include the antiproteinuric, as well. If you compare a blood test vs. urine test, then the urine is probably a much more reliable indicator because when the basement membrane is damaged, filtration is impaired such that the basement membrane between the podocyte processes no longer conserves plasma proteins and the amount lost, ‘leaked’ is present in the urine. The appearance of albumin (protein) in the urine is a ‘flag’ that loss of serum protein due to impaired renal function. Often, this is one of the earliest markers. Blood biomarkers have some variables that could result in misclassification of CKD stages. Protein leaking from the kidneys, is a direct correlate to the podocyte/basement-membrane damage. This is the gold-standard measure of endothelial function. I always like to use at least one blood marker (ideally CystatinC) in addition to the urine test, to facilitate extrapolating, “pinpointing” the true stage at baseline and where they are at follow-up.
I believe niacin is probably one of the best treatment options for a variety of chronic conditions/pathologies. CKD is a complex disease state. At its ‘core’, it is a vascular disease, but if you “hit all the right buttons” it is clearly possible to ‘drive’ CKD backwards.
With stage-5-CKD, a.k.a. end-stage renal disease (ESRD), the scarcity of donor organs is a primary challenge. The reality is usually that dialysis will be required for the rest of the patient’s life. That is a powerful motivator to the patient to consider niacin.
Ultimately my father’s CKD, reversed from stage 4 to stage 2. When the sum of all the data, connecting-the-dots with all the biomarkers, he was close to end stage renal disease as he was scheduled to have a first encounter with a nephrologist. So, he was likely headed to dialysis, sooner vs. later.
The Current State of CKD Treatment and the Importance of Addressing Multimorbidity
In regard to prevention, many physicians choose not to believe there is any way to prevent or reverse CKD. Unfortunately, most patients end up on dialysis, or at the very least their CKD continues to get worse.
Too often, a less than adequate job of correctly identifying pre-diabetes is implemented, early on in the CKD disease state. It is vitally important to have a method of measuring the glucose post-prandial (PPG) level at 1h and 2h post-glucose challenge (OGTT). Currently, this is the gold standard test for assessing pre-diabetes. There are blood biomarkers that have a VERY high level of precision determining the 1-hr PPG: 1,5-AG and AHB (Alpha-HydroxyButyrate).
Measures of fasting insulin, fasting glucose, and HbA1c can miss an unacceptably large number of pre-diabetics. The OGTT test, will reliably capture a pre-diabetes diagnosis. HOMA-IR (HOMA-IR; homeostasis model assessment as an index of insulin resistance) is an effective method to calculate and evaluate insulin resistance using conventional reference lab biomarkers: insulin levels, fasting glucose levels, and A1C.60,61 If you have these three, you can then calculate the HOMA-IR. This enables accurate documentation and validates spending the modest expense to do the proper tests.
As much as 70% of adults over the age of 30 do not have normal postprandial glucose (PPG). It’s that bad! They say it’s only 30% or 40%, but that’s likely based on poor statistics. In fact, during every year in the last several decades, the percentage of individuals over the age of 30 with obesity has risen. The antiquated Frederickson classification was based on cholesterol/triglyceride parameters, but we are presently in the ‘particle age’ of clinical lipidemia assessment. Like the Frederickson classification for lipid disorder sub-types (which was largely based on cholesterol measurements), current methods to assess the presence and severity of insulin-resistance (a.k.a. pre-diabetes) are essentially obsolete.
Another aspect to consider is multiple comorbidities. Modern medicine currently generally takes the approach of treating one condition at a time, but there are nearly always multiple disease symptoms present that are tightly associated and anything that can ultimately address this is going to result in the most effective therapies, ideally prior to the fulminant disease.
The Academy of Medical Sciences declared in 2018 that multimorbidity is the number one top priority in healthcare research.62 Estimates for a cure of cancer reveal that this would only increase lifespan by a mere three years on average because the associated co-morbidities were not addressed.63 Niacin, however, addresses so many common denominators for disparate diseases that the impact of niacin treatment for CKD/ESRD is likely to benefit many more indications, especially the number one killer, cardiovascular disease.
At the end of the day, it is the effect on all-cause mortality that matters the most for any treatment. After the termination of the Coronary Drug Project-CDP trial, it was determined that all-cause mortality was reduced by 11%, nine years after stopping niacin treatment (avg. dose 2.4 g/day).64 This may be a feat unparalleled in proven clinical medicine. By contrast, statin all-cause mortality data has yielded mixed results.
Conclusion
In over 25 documented individual cases of CKD stages 2 through 4, after initiation of a combination-therapy of supplements based on GFR, including 500 mg TID IR-niacin, over a three-month period, it was possible to improve their disease by at least one stage.
In basic and clinical research the evidence in favor of niacin for CKD is strong. Clinical research proves that the niacin is exceptionally well-suited to treatment and prevention of CKD, multimorbidity, and ultimately all-cause mortality.
Sampathkumar explained the current CKD treatment with niacin situation best:
Pharmaceutical industry driven large-scale studies are unlikely to be undertaken given the low-cost of niacin. David is up against the formidable Goliath of players promoting costly non-calcium containing phosphorus binders. It is time that international bodies like Kidney Disease, Improving Global Outcomes (KDIGO) take a call on usefulness of niacin as a low-cost, effective, and low pill burden agent for phosphorus reduction in CKD with multiple pleotropic benefits.29
Recommended Doses to Address Chronic Kidney Disease
Low-dose immediate release-niacin, 100 mg – 500 mg, 1 to 3x/day. No-flush niacin or niacinamide will have equal efficacy on lowering phosphorus levels, but negligible cardio-vascular benefits compared with standard niacin.
Sodium Bicarbonate (baking soda) 1.8 g/d (1/3 at lunch and 2/3 at dinner).
Calcium carbonate antacid pills (400-1000 mg elemental calcium or 2-4 gms antacid tablets) with food to bind phosphorous in food.
Low-Dose-Thyroid Supplementation (25-50 µg T4/Levothyroxine or ½ grain of Desiccated Thyroid).
Methyl Folate (0.8 g to 2 mg L-MethylFolate).
Recommended Additional Monitoring
A full panel of metabolic parameters [baseline and 90-day f/u] can also determine ‘collateral’ benefit[s], especially related to cardiovascular health:
Apo-B decreases
Apo-A1 increases (INTERHEART Study)
Lp(a) mass decreases
Lp-PLA2 decreases
MPO/myeloperoxidase| decreases
AST/ALT/GGT hepatic parameters improved
Symptomology/Signs-Symptoms: TIA; Chronic Angina; Claudication; Dyspnea upon Exertion.
The views of the authors, who are not physicians, are presented here for educational purposes. All readersare reminded to be sure to work with their own health care provider(s) before commencing this or any nutrition-based approach.
Stephen D. McConnell is a lipidemiologist and researcher with an MSc in cardiovascular and renal pathophysiology.
W. Todd Penberthy, PhD, specializes in writing about targeted pharmacotherapeutics, CME, and biomedical texts.